Objective: This study utilized shear wave elastography (SWE) to evaluate endometrial receptivity (ER) in cases of unexplained infertility (UI) following treatment with clomiphene citrate (CC). The aim was to establish a reliable imaging reference for clinical treatment. Methods: This investigation encompassed 68 patients with UI who attended our hospital from October 2023 to May 2024. Participants were allocated to either a CC group (28 participants) or a normal control (NC) group (40 participants) according to the treatment protocols they followed. During the LP phase (days 13-16) and the MP phase (6-9 days post-ovulation), both groups underwent transvaginal ultrasound and SWE assessments. The evaluated parameters included endometrial thickness (EMT), uterine artery parameters (UA-PI, UA-RI, UA-S/D), average endometrial elasticity (E-mean), and mean shear wave velocity (SWV-mean). Additionally, clinical pregnancy outcomes were tracked. Results: Significant variations were observed between the CC and NC groups in E-mean, SWV-mean, EMT, UA-PI, UA-RI, and UA-S/D during both evaluated phases, with statistical significance (P<0.05). Nevertheless, there were no significant variations found in clinical pregnancy rates among the groups (P>0.05). Significant statistical differences were observed in E- mean and SWV-mean between pregnant and non-pregnant patients within each group (P<0.05). Conclusions: After CC treatment, the endometrium in UI patients showed decreased thickness, increased hardness, reduced blood flow, and increased difficulty in implantation. Despite these effects, CC did not significantly impact clinical pregnancy rates. Future studies should expand the sample size to determine the threshold of endometrial hardness that optimally balances its effects.
| Published in | Clinical Medicine Research (Volume 13, Issue 6) |
| DOI | 10.11648/j.cmr.20241306.11 |
| Page(s) | 68-76 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Clomiphene Citrate, Endometrial Receptivity, Shear Wave Elastography, Unexplained Infertility
Groups | Age (years) | Year of infertility | BMI (kg/m2) | Follicle-stimulating hormone (mIU/mL) | Luteinizing hormone (mIU/mL) | Estradiol (ng/mL) |
|---|---|---|---|---|---|---|
CC (n=28) | 29.07±3.92 | 2.48±0.44 | 22.25±1.77 | 6.23±0.88 | 4.38±0.47 | 37.65 (37.18, 38.03) |
NC (n=40) | 29.23±4.12 | 2.45±0.32 | 22.91±2.00 | 5.91±0.73 | 4.58±0.70 | 37.30 (26.38, 46.80) |
Z/t | -0.154 | 0.296 | -1.417 | 1.666 | -1.307 | -0.237 |
P | 0.878a | 0.768a | 0.161a | 0.101a | 0.196a | 0.813b |
Groups | EMT (mm) | UA-PI | UA-RI | UA-S/D | E-mean (kPa) | SWV-mean (m/s) |
|---|---|---|---|---|---|---|
CC | ||||||
LPCC | 6.55 (5.53, 8.33) | 2.64 (2.30, 2.90) | 0.88 (0.85, 0.91) | 8.05 (6.51, 9.94) | 32.05 (19.53, 37.87) | 3.24 (2.53, 3.52) |
MPCC | 9.40 (8.50, 11.18) | 2.31 (1.85, 2.52) | 0.85 (0.78, 0.87) | 7.18 (6.55, 9.09) | 12.46 (7.28, 21.15) | 1.92 (1.62, 2.16) |
NC | ||||||
LPNC | 8.60 (7.93, 9.68) | 2.27 (2.07, 2.64) | 0.85 (0.81, 0.89) | 7.14 (5.38, 8.39) | 16.32 (11.95, 21.01) | 2.32 (1.98, 2.63) |
MPNC | 11.55 (10.43, 12.50) | 1.97 (1.74, 2.15) | 0.81 (0.77, 0.83) | 6.25 (5.37, 7.10) | 8.69 (6.84, 9.63) | 1.67 (1.37, 1.85) |
PLPCCvsLPNC | 0.000b | 0.003b | 0.018b | 0.034b | 0.000b | 0.000b |
PMPCCvsMPNC | 0.000b | 0.001b | 0.023b | 0.002b | 0.000b | 0.004b |
PLPCCvsMPCC | 0.000C | 0.000C | 0.002C | 0.030C | 0.000C | 0.000C |
PLPNCvsMPNC | 0.000C | 0.000C | 0.000C | 0.006C | 0.000C | 0.000C |
Groups | Cases (n) | Clinical pregnancy rate [n (%)] |
|---|---|---|
CC | 28 | 6 (21.4) |
NC | 40 | 5 (12.5) |
X2 | 0.422 | |
P | 0.516d |
Groups | EMT (mm) | UA-PI | UA-RI | UA-S/D | E-mean (kPa) | SWV-mean (m/s) |
|---|---|---|---|---|---|---|
CC | ||||||
PCC | 9.50 (9.03, 10.53) | 2.24 (1.68, 2.86) | 0.85 (0.76, 0.91) | 6.45 (5.24, 6.89) | 9.42 (8.41, 9.84) | 1.52 (1.39, 1.62) |
NCC | 9.40 (8.15, 11.58) | 2.31 (1.85, 2.52) | 0.85 (0.78, 0.87) | 7.83 (6.70, 9.20) | 13.48 (11.45, 22.94) | 1.97 (1.82, 2.53) |
NC | ||||||
PNC | 11.60 (10.35, 12.35) | 1.95 (1.79, 2.14) | 0.81 (0.77, 0.83) | 6.30 (5.10, 7.10) | 6.12 (5.39, 6.96) | 1.27 (1.18, 1.32) |
NNC | 11.50 (10.40, 12.60) | 1.97 (1.74, 2.15) | 0.81 (0.77, 0.83) | 6.25 (5.37, 7.10) | 8.85 (6.88, 10.38) | 1.68 (1.51, 1.97) |
PPCCvsNCC | 0.694b | 0.889b | 0.633b | 0.017b | 0.004b | 0.001b |
PPNCvsNNC | 0.854b | 0.413b | 0.226b | 0.919b | 0.000b | 0.004b |
CC | Clomiphene Citrate |
E2 | Estradiol |
E-mean | Mean Endometrial Elasticity |
EMT | Endometrial Thickness |
ER | Endometrial Receptivity |
FSH | Follicle-Stimulating Hormone |
HCG | Human Chorionic Gonadotropin |
LH | Luteinizing Hormone |
LP | Late-Proliferative Phase |
MP | Mid-Secretory Phase |
NC | Normal Control |
SWE | Shear Wave Elastography |
SWV-mean | Mean Shear Wave Velocities |
TVS | Transvaginal Ultrasonography |
UA-PI | Uterine Artery Pulsatility Index |
UA-RI | Uterine Artery Resistance Index |
UA-S/D | Uterine Artery Peak Systolic Velocity / End Diastolic Velocity |
UI | Unexplained Infertility |
| [1] | Carson, S. A., Kallen, A. N. Diagnosis and management of infertility: a review. JAMA. The Journal of the American Medical Association. 2021, 326(1), 65-76. |
| [2] | Lessey, B. A., Young, S. L. What exactly is endometrial receptivity? Fertility and Sterility. 2019, 111(4), 611-617. |
| [3] | Achache, H., Revel, A. Endometrial receptivity markers, the journey to successful embryo implantation. Human Reproduction Update. 2006, 12(6), 731-746. |
| [4] | Messaoudi, S., Kasmi, I. E., Bourdiec, A., Crespo, K., Bissonnette, L., Saint, C. L. 15 years of transcriptomic analysis on endometrial receptivity: what have we learnt? Fertility Research and Practice. 2019, 5(1), 9. |
| [5] | Inhorn, M. C., Patrizio, P. Infertility around the globe: new thinking on gender, reproductive technologies and global movements in the 21st century. Human Reproduction Update. 2015, 21(4), 411-426. |
| [6] | Franasiak, J. M., Forman, E. J., Hong, K. H., Werner, M. D., Upham, K. M., Treff, N. R., Scott Jr, R. T. The nature of aneuploidy with increasing age of the female partner: a review of 15,169 consecutive trophectoderm biopsies evaluated with comprehensive chromosomal screening. Fertility and Sterility. 2014, 101(3), 656-663. |
| [7] | Guideline Group on Unexplained Infertility, Romualdi, D., Ata, B., Bhattacharya, S., Bosch, E., Costello, M., Le Clef, N. Evidence-based guideline: unexplained infertility. Human Reproduction, 38(10), 1881-1890. Evidence-based guideline: unexplained infertility. Human Reproduction. 2023, 38(10), 1881-1890. |
| [8] | Sigrist, R. M., Liau, J., El Kaffas, A., Chammas, M. C., Willmann, J. K. Ultrasound elastography: review of techniques and clinical applications. Theranostics. 2017, 7(5), 1303. |
| [9] | Cheng, M. Q., Xian, M. F., Tian, W. S., Li, M. D., Hu, H. T., Li, W,. RGB Three-Channel SWE-Based Ultrasomics Model: Improving the Efficiency in Differentiating Focal Liver Lesions. Frontiers in Oncology. 2021, 11, 704218. |
| [10] | Yu, C. C., Jiao, Y., Wang, J. J., Zhao, X. S., Chen, L. Preliminary application of real-time shear wave elastography to evaluate endometrial receptivity and predict pregnancy outcome. Technology and Health Care. 2024, (Preprint), 1-8. |
| [11] | Li, Z. Y., Cai, L., Zhang, Z. J., Zou, H. R., He, M., Qin, M. L., Wang, H. Evaluation of endometrial receptivity in women with unexplained infertility by shear wave elastography. Insights into Imaging. 2024, 15(1), 85. |
| [12] | Karaoğlan, Ö., Kuyucu, Y., Ürünsak, İ. F., Gümürdülü, D., Tap, Ö. Morphological features of the secretory phase endometrium in women with unexplained infertility. Ultrastructural Pathology. 2021, 45(3), 243-256. |
| [13] | Stanziano, A., Bianchi, F. P., Caringella, A. M., Cantatore, C., D'Amato, A., Vitti, A. The use of real time strain endometrial elastosonography plus endometrial thickness and vascularization flow index to predict endometrial receptivity in IVF treatments: a pilot study. BMC Medical Imaging. 2023, 23(1), 130. |
| [14] | Rani, K. U., Gupta, J., Bajaj, B., Das, B., Marwah, S. Comparative Evaluation of Follicular Development and Endometrial Thickness in Spontaneous and Clomiphene Citrate Induced Cycle in Unexplained Infertility. Group. 2020, 15(18), 19-22. |
| [15] | Cetin, E., Siblini, H., Al-Hendy, A. What is the mechanism of poor endometrial proliferation in patients with unexplained infertility after clomiphene citrate treatment?. The Journal of Clinical Endocrinology & Metabolism. 2021, 106(11), e4776-e4777. |
| [16] | Gingold, J. A., Lee, J. A., Rodriguez, P. J., Whitehouse, M. C., Sandler, B., Grunfeld, L., Copperman, A. B. Endometrial pattern, but not endometrial thickness, affects implantation rates in euploid embryo transfers. Fertility and Sterility. 2015, 104(3), 620-628. |
| [17] | Glujovsky, D., Pesce, R., Sueldo, C., Retamar, A. M. Q., Hart, R. J., Ciapponi, A. Endometrial preparation for women undergoing embryo transfer with frozen embryos or embryos derived from donor oocytes. Cochrane Database of Systematic Reviews. 2020, (10), 31-40. |
| [18] | Montenegro, I. S., Kuhl, C. P., Schneider, R. D. A., Zachia, S. D. A., Passos, E. P. Use of clomiphene citrate protocol for controlled ovarian stimulation impairs endometrial maturity. JBRA Assisted Reproduction. 2021, 25(1), 90. |
| [19] | Basir, G. S., O, W. S., Yu Ng, E. H., Ho, P. C. Morphometric analysis of peri-implantation endometrium in patients having excessively high oestradiol concentrations after ovarian stimulation. Human Reproduction. 2001, 16(3), 435-440. |
| [20] | Zackrisson, U., Brännström, M., Granberg, S., Janson, P. O., Collins, W. P., Bourne, T. H. Acute effects of a transdermal nitric oxide donor on perifollicular and intrauterine blood flow. Ultrasound in Obstetrics and Gynecology: The Official Journal of the International Society of Ultrasound in Obstetrics and Gynecology. 1998, 12(1), 50-55. |
| [21] | Zaidi, J. Blood flow changes in the ovarian and uterine arteries in women with normal and polycystic ovaries. Human Fertility. 2000, 3(3), 194-198. |
| [22] | Leah, H. B., Fritz, M. A., San-Pin, W., Lingwen, Y., Suzanna, K., Tianyuan, W. Poor endometrial proliferation after clomiphene is associated with altered estrogen action. The Journal of Clinical Endocrinology & Metabolism. 106(9), 2547-2565. |
| [23] | Karizbodagh, M. P., Rashidi, B., Sahebkar, A., Masoudifar, A., Mirzaei, H. Implantation window and angiogenesis. Journal of Cellular Biochemistry. 2017, 118(12), 4141-4151. |
| [24] | Zhang, Y., Lin, X., Dai, Y., Hu, X., Zhu, H., Jiang, Y. Endometrial stem cells repair injured endometrium and induce angiogenesis via AKT and ERK pathways. Reproduction. 2016, 152(5), 389-402. |
| [25] | Jamal, A., Abbasalizadeh, F., Vafaei, H., Marsoosi, V., Eslamian, L. Multicenter screening for adverse pregnancy outcomes by uterine artery Doppler in the second and third trimester of pregnancy. Medical ultrasonography. 2013, 15(2), 95-100. |
| [26] | Tong, R., Zhou, Y., He, Q., Zhuang, Y., Zhou, W., Xia, F. Analysis of the guidance value of 3D ultrasound in evaluating endometrial receptivity for frozen-thawed embryo transfer in patients with repeated implantation failure. Annals of Translational Medicine. 2020, 8(15). |
| [27] | Sereepapong, W., Suwajanakorn, S., Triratanachat, S., Sampatanukul, P., Reinprayoon, D. Effects of clomiphene citrate on the endometrium of regularly cycling women. Fertility and Sterility. 2000, 73(2), 287-291. |
| [28] | Cook, C. L., Schroeder, J. A., Yussman, M. A., Sanfilippo, J. S. Induction of luteal phase defect with clomiphene citrate. American Journal of Obstetrics and Gynecology. 1984, 149(6), 613-616. |
| [29] | Daly, D. C., Maslar, I. A., Riddick, D. H. Prolactin production during in vitro decidualization of proliferative endometrium. American Journal of Obstetrics and Gynecology. 1983, 145(6), 672-678. |
| [30] | Li, M., Zhu, X., Wang, L., Fu, H., Zhao, W., Zhou, C., Yao, B. Evaluation of endometrial receptivity by ultrasound elastography to predict pregnancy outcome is a non-invasive and worthwhile method. Biotechnology and Genetic Engineering Reviews, 2023, 08, 1-15. |
| [31] | Stanziano, A., Bianchi, F. P., Caringella, A. M., Cantatore, C., D'Amato, A., Vitti, A. The use of real time strain endometrial elastosonography plus endometrial thickness and vascularization flow index to predict endometrial receptivity in IVF treatments: a pilot study. BMC Medical Imaging. 2023, 23(1), 130. |
| [32] | Hughes, E., Brown, J., Collins, J. J., Vanderkerchove, P. (2010). Clomiphene citrate for unexplained subfertility in women. Cochrane Database of Systematic Reviews. 2000, 65(1), CD000057. |
APA Style
He, M., Li, Z., Cai, L., Xie, T., Cui, L., et al. (2024). Evaluation of Endometrial Receptivity in Unexplained Infertility After Clomiphene Citrate by Shear Wave Elastography. Clinical Medicine Research, 13(6), 68-76. https://doi.org/10.11648/j.cmr.20241306.11
ACS Style
He, M.; Li, Z.; Cai, L.; Xie, T.; Cui, L., et al. Evaluation of Endometrial Receptivity in Unexplained Infertility After Clomiphene Citrate by Shear Wave Elastography. Clin. Med. Res. 2024, 13(6), 68-76. doi: 10.11648/j.cmr.20241306.11
@article{10.11648/j.cmr.20241306.11,
author = {Mei He and Zheng-ying Li and Lu Cai and Tao Xie and Li-qing Cui and Hui Wang},
title = {Evaluation of Endometrial Receptivity in Unexplained Infertility After Clomiphene Citrate by Shear Wave Elastography
},
journal = {Clinical Medicine Research},
volume = {13},
number = {6},
pages = {68-76},
doi = {10.11648/j.cmr.20241306.11},
url = {https://doi.org/10.11648/j.cmr.20241306.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cmr.20241306.11},
abstract = {Objective: This study utilized shear wave elastography (SWE) to evaluate endometrial receptivity (ER) in cases of unexplained infertility (UI) following treatment with clomiphene citrate (CC). The aim was to establish a reliable imaging reference for clinical treatment. Methods: This investigation encompassed 68 patients with UI who attended our hospital from October 2023 to May 2024. Participants were allocated to either a CC group (28 participants) or a normal control (NC) group (40 participants) according to the treatment protocols they followed. During the LP phase (days 13-16) and the MP phase (6-9 days post-ovulation), both groups underwent transvaginal ultrasound and SWE assessments. The evaluated parameters included endometrial thickness (EMT), uterine artery parameters (UA-PI, UA-RI, UA-S/D), average endometrial elasticity (E-mean), and mean shear wave velocity (SWV-mean). Additionally, clinical pregnancy outcomes were tracked. Results: Significant variations were observed between the CC and NC groups in E-mean, SWV-mean, EMT, UA-PI, UA-RI, and UA-S/D during both evaluated phases, with statistical significance (P0.05). Significant statistical differences were observed in E- mean and SWV-mean between pregnant and non-pregnant patients within each group (P<0.05). Conclusions: After CC treatment, the endometrium in UI patients showed decreased thickness, increased hardness, reduced blood flow, and increased difficulty in implantation. Despite these effects, CC did not significantly impact clinical pregnancy rates. Future studies should expand the sample size to determine the threshold of endometrial hardness that optimally balances its effects.
},
year = {2024}
}
TY - JOUR T1 - Evaluation of Endometrial Receptivity in Unexplained Infertility After Clomiphene Citrate by Shear Wave Elastography AU - Mei He AU - Zheng-ying Li AU - Lu Cai AU - Tao Xie AU - Li-qing Cui AU - Hui Wang Y1 - 2024/11/22 PY - 2024 N1 - https://doi.org/10.11648/j.cmr.20241306.11 DO - 10.11648/j.cmr.20241306.11 T2 - Clinical Medicine Research JF - Clinical Medicine Research JO - Clinical Medicine Research SP - 68 EP - 76 PB - Science Publishing Group SN - 2326-9057 UR - https://doi.org/10.11648/j.cmr.20241306.11 AB - Objective: This study utilized shear wave elastography (SWE) to evaluate endometrial receptivity (ER) in cases of unexplained infertility (UI) following treatment with clomiphene citrate (CC). The aim was to establish a reliable imaging reference for clinical treatment. Methods: This investigation encompassed 68 patients with UI who attended our hospital from October 2023 to May 2024. Participants were allocated to either a CC group (28 participants) or a normal control (NC) group (40 participants) according to the treatment protocols they followed. During the LP phase (days 13-16) and the MP phase (6-9 days post-ovulation), both groups underwent transvaginal ultrasound and SWE assessments. The evaluated parameters included endometrial thickness (EMT), uterine artery parameters (UA-PI, UA-RI, UA-S/D), average endometrial elasticity (E-mean), and mean shear wave velocity (SWV-mean). Additionally, clinical pregnancy outcomes were tracked. Results: Significant variations were observed between the CC and NC groups in E-mean, SWV-mean, EMT, UA-PI, UA-RI, and UA-S/D during both evaluated phases, with statistical significance (P0.05). Significant statistical differences were observed in E- mean and SWV-mean between pregnant and non-pregnant patients within each group (P<0.05). Conclusions: After CC treatment, the endometrium in UI patients showed decreased thickness, increased hardness, reduced blood flow, and increased difficulty in implantation. Despite these effects, CC did not significantly impact clinical pregnancy rates. Future studies should expand the sample size to determine the threshold of endometrial hardness that optimally balances its effects. VL - 13 IS - 6 ER -
Department of Ultrasound, University-Town Hospital of Chongqing Medical University, Chongqing, China
Department of Ultrasound, University-Town Hospital of Chongqing Medical University, Chongqing, China
Department of Ultrasound, University-Town Hospital of Chongqing Medical University, Chongqing, China
Department of Ultrasound, University-Town Hospital of Chongqing Medical University, Chongqing, China
Department of Ultrasound, University-Town Hospital of Chongqing Medical University, Chongqing, China
Department of Ultrasound, University-Town Hospital of Chongqing Medical University, Chongqing, China
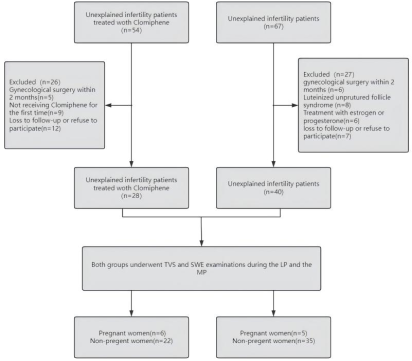
Figure 1. Flow chart of the study population. TVS transvaginal ultrasonography. SWE shear wave elastography. LP late-proliferative phase. MP mid-secretory phase.
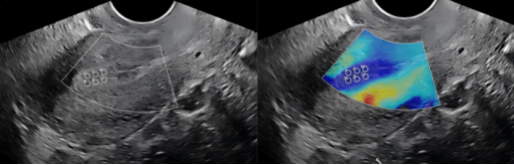
Figure 2. Sonographic image of endometrial elastography measurement. In a standard sagittal section of the uterus, the middle and upper segment of the endometrium is completely covered by the white sampling frame. The white circles represent the six sampling sites for SWE.
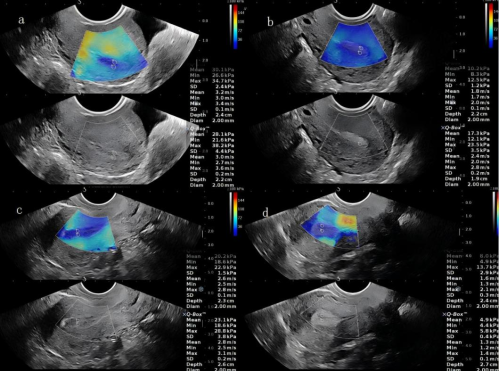
Figure 3. Representative images of one person in group CC during LP(a) and MP(b). a In the LPCC group, the mean elasticity (E-mean) and mean shear wave velocity (SWV-mean) at the two ROIs of the upper endometrial segments were 30.1 kPa and 28.1 kPa and 3.2 m/s and 3.0 m/s. b In the MPCC group, the E-mean and SWV-mean at the two ROIs of the upper endometrial segments were 10.2 kPa and 17.3 kPa and 1.8 m/s and 2.4 m/s. Representative images of one person in group NC during LP(c) and MP(d). c In the LPNC group, the mean elasticity (E-mean) and mean shear wave velocity (SWV-mean) at the two ROIs of the upper endometrial segments were 20.2 kPa and 23.1 kPa and 2.6 m/s and 2.8 m/s. d In the MPNC group, the E-mean and SWV-mean at the two ROIs of the upper endometrial segments were 8.0 kPa and 4.9 kPa and 1.6 m/s and 1.3 m/s.

